
For many years, traditional total shoulder replacement has been a standard procedure for treating shoulder arthritis where the rotator cuff is intact. However, a specific set of conditions, particularly those involving a severely damaged or non-functional rotator cuff, necessitated a different approach. Reverse shoulder replacement fundamentally alters the mechanics of the shoulder joint to provide a new potential path to pain relief and functional restoration for patients who previously had limited alternatives.
Key Takeaways
- The reverse shoulder replacement is a specialized form of shoulder replacement that reverses the natural ball-and-socket anatomy of the shoulder joint.
- By reversing the anatomy, a reverse shoulder replacement shifts the center of rotation and allows the deltoid muscle to compensate for the damaged rotator cuff.
- Recovery is a structured process typically involving a period of immobilization followed by extensive, guided physical therapy, with functional improvement often continuing for up to a year or more.
Understanding the Shoulder Joint: A Foundation for Replacement
The shoulder is a complex structure composed of three bones: the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone). The glenohumeral joint is a ball-and-socket joint. The “ball” is the rounded head of the humerus, and the “socket” is the shallow, cup-shaped glenoid on the scapula.
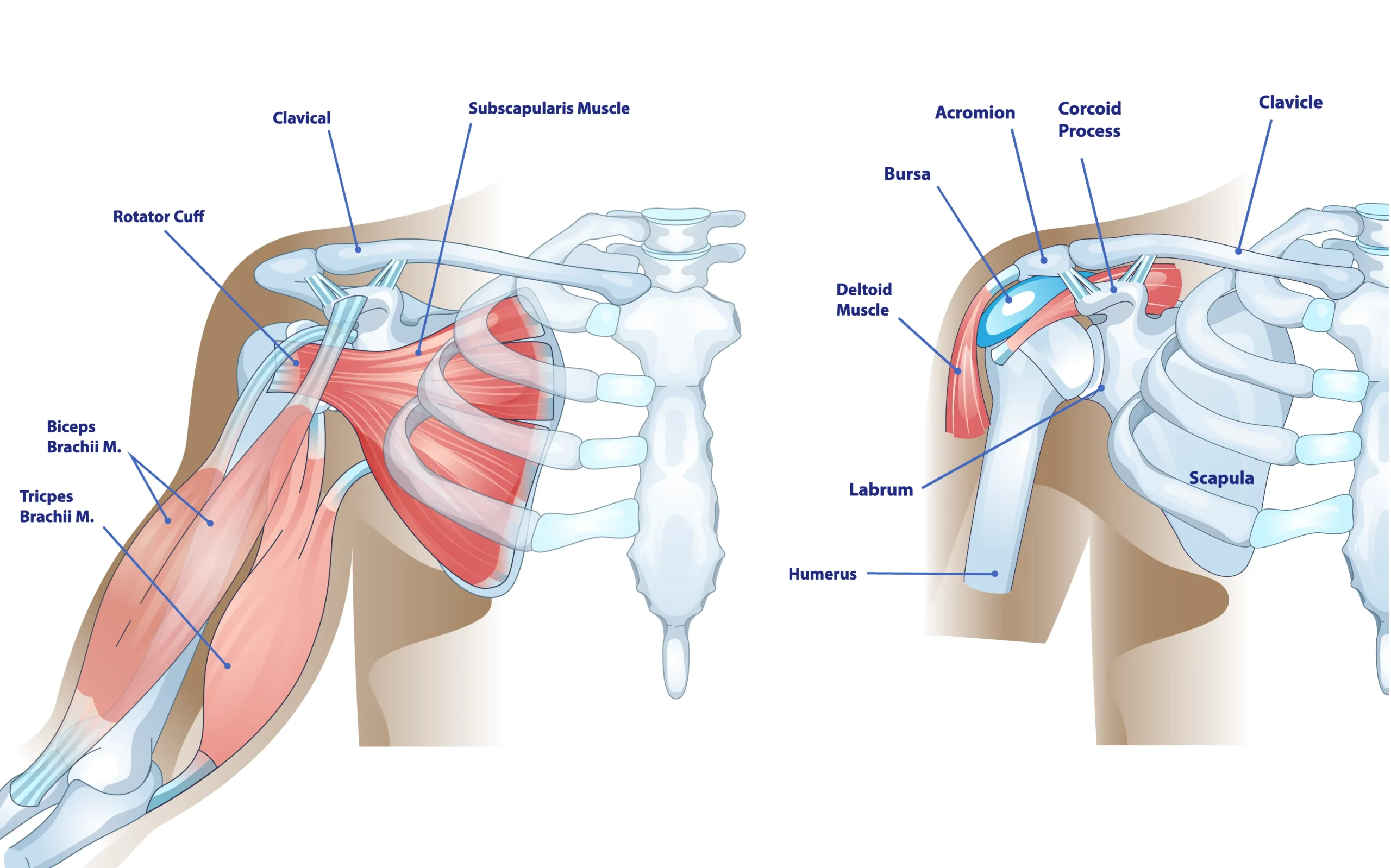
In a healthy shoulder, this joint is stabilized and moved by two primary muscle groups. The rotator cuff is a group of four tendons and their associated muscles that surround the joint, providing fine control, stability, and the initial power for lifting and rotating the arm. The deltoid muscle covers the shoulder and provides force for lifting the arm overhead. The rotator cuff keeps the humeral head (the ball) centered in the glenoid (the socket) during movement, preventing it from migrating upward when the deltoid contracts.
The Conditions That Lead to Reverse Shoulder Replacement
Traditional total shoulder replacement may be effective when the pain is caused by arthritis and the rotator cuff is still intact and functional. However, certain conditions compromise the rotator cuff, making a traditional replacement ineffective. The reverse shoulder replacement was developed to address these challenging scenarios.
Cuff Tear Arthropathy (CTA)
Cuff tear arthropathy is a form of shoulder arthritis that develops as a direct consequence of a massive rotator cuff tear. When the rotator cuff is torn and non-functional, it can no longer hold the humeral head centered in the glenoid socket. The deltoid muscle, when activated, pulls the humeral head upward (superiorly) until it rubs against the acromion(the bony roof of the shoulder blade). This abnormal contact and friction cause rapid, severe wear and tear on the joint cartilage.
Massive and Irreparable Rotator Cuff Tears
Even without advanced arthritis, a massive rotator cuff tear that cannot be surgically repaired may be an indication for reverse shoulder replacement. The goal here is to restore the ability to lift the arm (active elevation) and relieve the pain caused by the instability and abnormal mechanics.
Complex Fractures
Severe, complex fractures of the proximal humerus (the top of the arm bone), particularly in older patients with poor bone quality, may be treated with a reverse shoulder replacement. For many patients, this may offer a more reliable path to functional recovery compared to attempting a complex fixation.
The Reverse Shoulder Replacement Procedure
The surgery is a major orthopedic procedure, typically performed under general anesthesia, often supplemented with a regional nerve block to manage post-operative pain.
In an anatomic shoulder replacement, the implant replicates the shoulder’s natural structure: the ball is placed on the top of the humerus (the arm bone), and the socket is positioned on the glenoid (part of the shoulder blade). In a reverse shoulder replacement, these positions are switched: the ball is attached to the glenoid, and the socket is fixed to the humerus. This reversal allows the deltoid muscle, rather than the damaged rotator cuff, to power arm movement.
Recovery and Rehabilitation: The Road to Function
Recovery from a reverse shoulder replacement is a structured, multi-phase process that requires commitment from the patient. The goal of rehabilitation is to protect the healing tissues, regain motion, and strengthen the deltoid muscle. Specific timelines and steps may vary between patients.
Phase 1: Protection
- Immobilization: The arm is typically placed in a sling to protect the surgical site and the healing soft tissues.
- Initial Therapy: The focus is on protecting the repair and allowing the soft tissues to heal. Patients are generally restricted from active movement of the shoulder (lifting the arm on their own). Passive range of motion exercises (where the therapist or the patient’s other arm moves the operated arm) may be started gently to prevent stiffness.
- Restrictions: Strict adherence to the surgeon’s restrictions is essential. This typically includes no lifting, no pushing, and no sudden movements.
Phase 2: Active Range of Motion
- Transition: Once the surgeon determines that the soft tissues have healed sufficiently, the patient transitions to active range of motion exercises. This is the phase where the patient begins to use their deltoid muscle to lift the arm.
- Focus: Physical therapy focuses on regaining active elevation and external rotation, guided by the specific surgical approach and the patient’s progress.
Phase 3: Strengthening and Functional Return
- Goal: The final phase focuses on strengthening the deltoid and other surrounding muscles to maximize functional use of the arm.
- Activities: Patients may work on exercises to improve strength, endurance, and coordination, preparing them for a return to daily activities and, eventually, low-impact sports or hobbies.
- Long-Term Improvement: While functional gains are often seen within the first six months, the strength and movement of the shoulder can continue to improve for up to a year or even longer post-surgery.
Summary
By reversing the ball-and-socket mechanism, the reverse shoulder replacement procedure harnesses the power of the deltoid muscle with the goal of restoring active arm elevation and providing pain relief. The decision to undergo this surgery requires careful consideration of the indications, the surgical process, and the commitment to a structured rehabilitation program. Consulting with an experienced shoulder specialist specializing in shoulder arthroplasty is the first step in determining if this advanced procedure is the right choice for your specific condition.
Frequently Asked Questions (FAQ)
Will I be able to lift my arm over my head after the surgery?
A goal of the reverse shoulder replacement is to restore the ability to actively lift the arm (active elevation), which is often limited or impossible before surgery due to the non-functional rotator cuff. Many patients achieve the ability to lift their arm to shoulder height or higher, significantly improving their ability to perform daily activities like reaching for objects or getting dressed. However, achieving full, overhead motion, especially with heavy lifting, is not always guaranteed and may be restricted to protect the implant.
How painful is the recovery process?
Many patients find that the most intense pain subsides within the first few days to a week. The pain gradually transitions into a manageable discomfort that may be addressed through physical therapy and continued medication as needed.
Are there any activities I should avoid after a reverse shoulder replacement?
Yes, there are typically long-term restrictions designed to protect the implant and maximize its longevity. While the specific restrictions can vary by surgeon, common recommendations include avoiding heavy lifting and high-impact activities. Your surgeon and physical therapist will provide a detailed list of activities to avoid and will guide you on how to safely return to a fulfilling and active lifestyle.




