
The shoulder joint is one of the most mobile joints in the human body, allowing for an incredible range of motion that is essential for countless daily activities. This complexity, however, also makes it susceptible to wear, tear, and disease. When chronic pain and loss of function in the shoulder reach a point where non-surgical treatments no longer provide adequate relief, a procedure known as total shoulder replacement may be recommended. This surgical intervention involves replacing the damaged surfaces of the shoulder joint with prosthetic components, with the primary goal of alleviating pain and restoring function.
Key Takeaways
- The primary goal of total shoulder replacement is to relieve chronic, debilitating shoulder pain and restore functional movement that has been lost due to joint damage.
- A common indication for the surgery is severe shoulder arthritis, such as osteoarthritis, rheumatoid arthritis, or post-traumatic arthritis, where the joint’s smooth cartilage lining has worn away.
- A structured rehabilitation program, which typically includes dedicated physical therapy, supports a successful outcome.
The Anatomy of the Shoulder: A Complex Ball-and-Socket Joint
The shoulder, or glenohumeral joint, is a highly complex structure that facilitates the arm’s movement in virtually every direction, making it the most mobile joint in the body.
The joint is formed by three primary bones: the humerus (the long bone of the upper arm), the scapula (the shoulder blade), and the clavicle (the collarbone). The glenohumeral joint itself is a ball-and-socket configuration. The “ball” is the rounded top of the humerus, known as the humeral head. The “socket” is a shallow depression on the scapula called the glenoid.
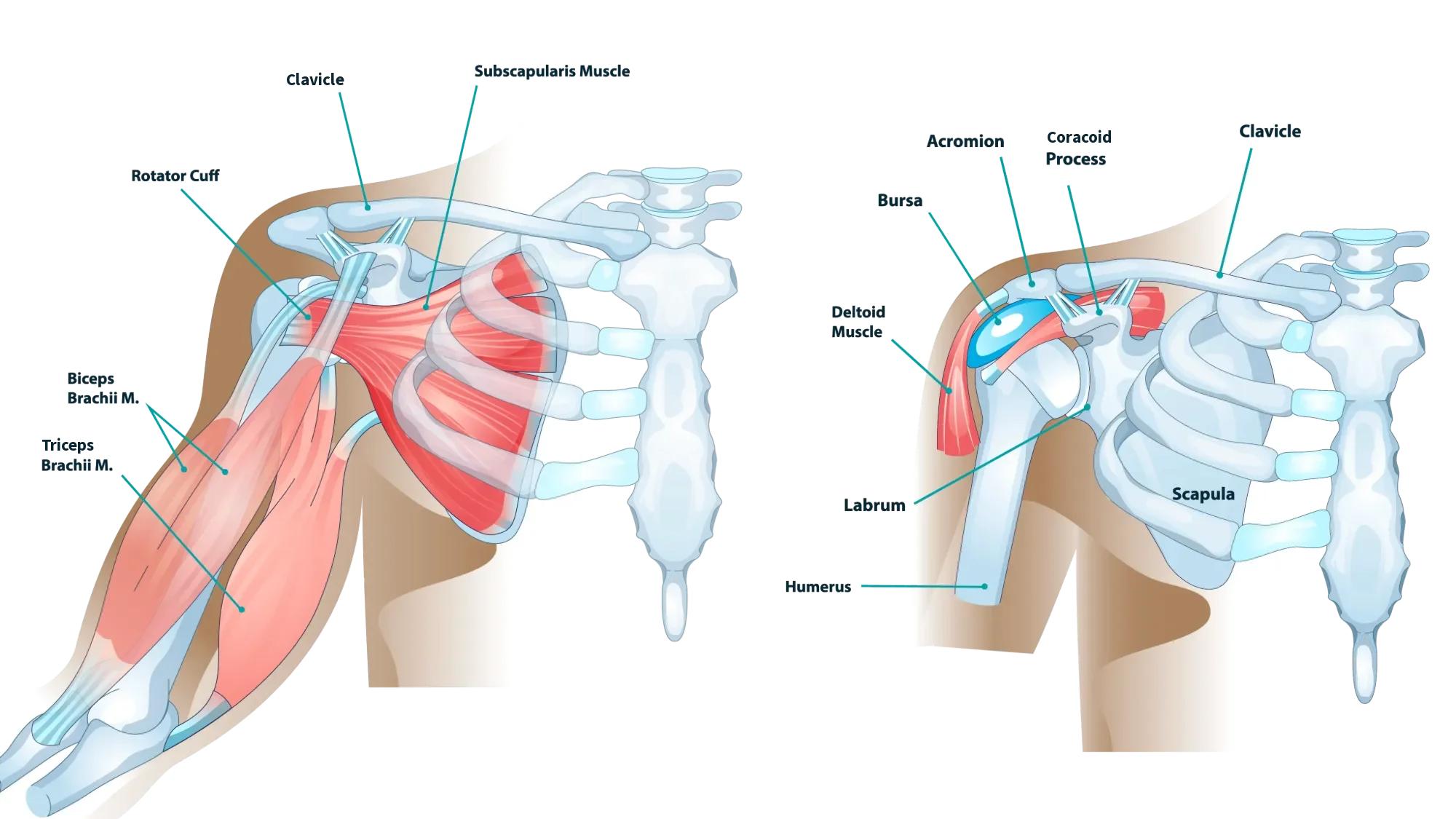
In a healthy shoulder, both the humeral head and the glenoid are covered with a smooth, resilient tissue called articular cartilage. This cartilage acts as a cushion and a low-friction surface, allowing the bones to glide against each other during movement. Surrounding and stabilizing this joint is a group of tendons and muscles known as the rotator cuff. The rotator cuff not only stabilizes the joint but also initiates and controls much of the shoulder’s movement.
Indications for Surgery: When the Cartilage Wears Away
Oftentimes, non-surgical treatment options such as medications and physical therapy will be attempted first before surgery is recommended. An experienced orthopedic surgeon can evaluate your condition and guide if total shoulder replacement may be an effective option. The primary reason a surgeon may recommend a total shoulder replacement is the presence of severe, chronic shoulder pain and functional limitation caused by the deterioration of the articular cartilage. This deterioration is broadly categorized as arthritis.
Osteoarthritis (Wear-and-Tear Arthritis)
Osteoarthritis, often referred to as “wear-and-tear” arthritis, is the most common reason for total shoulder replacement. Over many years of use, the articular cartilage on the humeral head and glenoid gradually may thin and break down. As the cartilage wears away, the protective space between the bones decreases and may lead to bone-on-bone friction. This friction can cause pain, stiffness, and a grinding sensation, limiting the ability to perform simple tasks like reaching, dressing, or sleeping comfortably.
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a systemic, autoimmune disease where the body’s immune system mistakenly attacks the lining of the joints, including the shoulder. This attack produces inflammatory chemicals that can destroy the articular cartilage and erode the underlying bone.
Post-Traumatic Arthritis
Post-traumatic arthritis develops following a significant injury to the shoulder, such as a severe fracture, a dislocation, or a major ligament or rotator cuff tear. Even after the initial injury has healed, the damage to the joint surfaces can lead to inconsistencies and irregularities that accelerate the wear-and-tear process, causing arthritis to develop years later.
The Procedure: Total Shoulder Replacement
The anatomic total shoulder replacement procedure is designed to replicate the natural structure of the shoulder joint. It is generally an option when the patient has severe arthritis but an intact and functional rotator cuff. If the patient has an irreparable or dysfunctional rotator cuff, reverse shoulder replacement may be recommended instead. The goal of the anatomic total shoulder replacement is to restore the joint’s natural alignment and anatomy.

In a total shoulder replacement, the damaged humeral head (the ball) is removed and replaced with a metal ball component. This component is typically attached to a stem that is inserted down the center of the humerus. Modern advancements have led to the development of short-stem or stemless humeral components, which are designed to preserve more of the patient’s natural bone. The damaged glenoid (the socket) is resurfaced with a smooth, high-density polyethylene (plastic) component. This component is cemented or fixed into the glenoid bone.
The Day of Surgery
On the day of the procedure, the patient will be admitted to the hospital or a surgery center. Total shoulder replacement is frequently performed under general anesthesia. The anesthesiologist will discuss options, which may include a local nerve block (interscalene block) to provide targeted pain relief in the shoulder and arm immediately following the operation.
The operation typically takes between one and three hours. The surgeon makes an incision, carefully navigates the surrounding muscles and tendons, removes the damaged bone and cartilage, and implants the prosthetic components.
Immediately after the surgery, the patient is moved to a recovery area where they are monitored as the anesthesia wears off. The surgeon will communicate the outcome of the procedure and recovery instructions to the patient’s family or friends.
The Recovery and Rehabilitation Journey
Recovery from total shoulder replacement is a marathon, not a sprint, and it requires patience and consistent effort. Timelines and exact instructions may vary based on the patient, but below we’ll detail a general phased approach.
Phase 1: Protection and Passive Motion
The initial phase focuses on protecting the healing tissues and allowing the joint to begin its recovery.
- Sling Use: The arm is typically kept in a sling for several weeks to immobilize the joint and protect the surgical site.
- Passive Range of Motion (PROM): Physical therapy often begins soon after surgery. During this phase, the therapist moves the patient’s arm without the patient using their own muscles. This is important for preventing stiffness.
- Daily Activities: Patients may expect to perform light daily activities, such as eating and dressing, with assistance or using the non-operative arm.
Phase 2: Active Motion and Early Strengthening
Once the surgeon determines that the soft tissues have healed sufficiently, the patient may transition to active movement.
- Active Range of Motion (AROM): The patient begins to move their own arm using their muscles.
- Light Strengthening: Gentle strengthening exercises are introduced to rebuild the muscle power lost during the period of immobilization. This phase focuses on restoring functional movement and control.
Phase 3: Advanced Strengthening and Return to Activity
The final phase is dedicated to maximizing strength, endurance, and functional return.
- Intensive Strengthening: The rehabilitation program progresses to more aggressive strengthening exercises.
- Return to Activity: Many patients return to light daily activities within a few weeks to a couple of months. Return to more demanding activities, such as golf, swimming, or light recreational sports, typically occurs after three to six months, provided the surgeon and therapist approve. It is important to note that high-impact activities or heavy, repetitive lifting may be discouraged long-term to protect the longevity of the implant.
Summary
Total shoulder replacement represents a well-established treatment for severe, debilitating shoulder arthritis and other complex shoulder conditions. It is a procedure that has evolved significantly, with modern techniques and implant designs focused on anatomical restoration, bone preservation, and durability.
If considering this procedure, patients are strongly encouraged to seek consultation with an orthopedic surgeon who specializes in shoulder replacement. A detailed discussion may ensure that questions are answered, the patient’s unique anatomy and condition are fully assessed, and an appropriate treatment plan is developed.
Frequently Asked Questions
How long does the total shoulder replacement surgery take?
The surgical procedure itself typically takes between one and three hours, depending on the complexity of the case and whether it is an anatomic or reverse replacement. This time does not include the pre-operative preparation or the post-operative recovery room time.
When can I start driving again?
The ability to drive is dependent on several factors, including which arm was operated on and whether you are taking narcotic pain medication. Generally, patients are advised to avoid driving for at least four to eight weeks, or until they have regained sufficient strength and range of motion, and are no longer taking prescription pain medication. Your surgeon can provide specific instructions, tailored to you.
How painful is recovery after surgery?
Some pain and discomfort are normal during the first few weeks, but modern pain-management techniques, including nerve blocks and medications, help keep it manageable. Pain generally improves steadily as healing progresses and motion returns.
Can I sleep on my operated side after surgery?
Patients are typically advised to avoid sleeping on the operative side for several weeks to protect the repair and reduce discomfort. Using pillows to support the arm in a semi-reclined or propped position can improve comfort during early recovery.




